Health care, single payer and the U.S.
Health care in the United States has several defining characteristics: it's extremely effective and high quality for the wealthy, difficult to receive for the poor, and extraordinarily cost inefficient and expensive as a system. Everyone wants to stop the skyrocketing cost of the health care system, many want to establish universal coverage. The first step has to be to control costs, and the best way to do that is with a single payer health care system.
The current system is patchwork and somewhat ad hoc, a mixture of public and private facilities providing care with a mixture of public and private funds. This fragmented system is different in every state and every community, built based on local priorities and resources yet straining almost everywhere to keep from falling apart. Politicians in the last two years have debated many strategies for reform, focusing on extending access to health care to more of the people who need it. That is a noble and just goal, but it has a fatal flaw: even as it is, the health care system is more expensive than we can afford. The first priority of reform should be to control and reduce costs, and the only way to make substantial and quick progress against the cost of delivering health care is to adopt a single payer system.
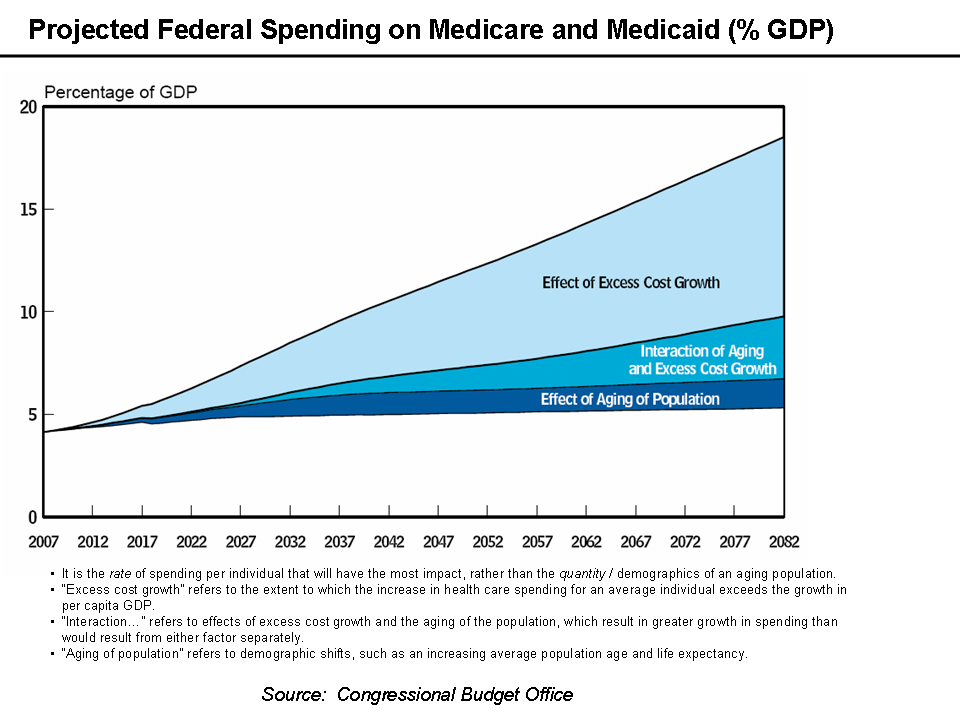 According to the federal government we spent $2.2 trillion on health care in 2008, an increase of 4.4% over 2007 and a slower rate than normal – yet still more than double the rate of inflation. The Centers for Medicaid & Medicare (CMS) predicts that by 2017 health care spending will account for nearly 20% of gross domestic product. At the same time, in 2008 the United States spent $1.40 for every $1 raised in revenue and added over $1 trillion to the national public debt. Opponents of nationalizing health insurance argue that while the United States spends a great deal more money per person on health care, the quality of care provided is unequaled in the world. Indeed, statistically the United States ranks first in the world for the responsiveness of the health care system; necessary care is provided much more quickly here than it is in other countries with a national, universal system. Others point to the distribution of spending in the United States and see an opportunity to reduce costs by improving access to primary and routine care, reducing the need for more intense and expensive hospital stays. If this were possible it might be a critical element of reform – $782 billion, or 35% of all spending, pays for hospital care. This strategy relies on changing the behavior of consumers, and while there are no definitive studies either way some have suggested that greater preventive care does not reduce the total costs of health care long-term. The fact remains that even during the greatest recession since the 1930s, the cost of health care is growing at an unsustainable rate that makes either reform or collapse inevitable.
According to the federal government we spent $2.2 trillion on health care in 2008, an increase of 4.4% over 2007 and a slower rate than normal – yet still more than double the rate of inflation. The Centers for Medicaid & Medicare (CMS) predicts that by 2017 health care spending will account for nearly 20% of gross domestic product. At the same time, in 2008 the United States spent $1.40 for every $1 raised in revenue and added over $1 trillion to the national public debt. Opponents of nationalizing health insurance argue that while the United States spends a great deal more money per person on health care, the quality of care provided is unequaled in the world. Indeed, statistically the United States ranks first in the world for the responsiveness of the health care system; necessary care is provided much more quickly here than it is in other countries with a national, universal system. Others point to the distribution of spending in the United States and see an opportunity to reduce costs by improving access to primary and routine care, reducing the need for more intense and expensive hospital stays. If this were possible it might be a critical element of reform – $782 billion, or 35% of all spending, pays for hospital care. This strategy relies on changing the behavior of consumers, and while there are no definitive studies either way some have suggested that greater preventive care does not reduce the total costs of health care long-term. The fact remains that even during the greatest recession since the 1930s, the cost of health care is growing at an unsustainable rate that makes either reform or collapse inevitable.

The United States spends more on health care each year, in absolute terms and as a percentage of gross domestic product (GDP, 16%), than any other country in the United Nations except tiny East Timor. Yet it's the only major industrialized nation in the world that does not ensure that all of its citizens have at least some health care coverage. As a result, life expectancy for US citizens lags behind the entire developed world, as does its infant mortality rate -- a 2000 analysis by the World Health Organization (WHO) put the US system 72nd in overall health. The delivery of health care in the United States is most often compared to the systems of Canada and England, and many studies have compared both quality and cost between them. There are many areas of criticism for both of the national health plans; both systems are known in the United States for comparatively long waits for some procedures, for not covering some expensive treatments and for not paying physicians and nurses as well. Additionally, direct cost comparisons between the United States and England can be misleading because of differences in the distribution of people – England is comparatively dense and urban, allowing for a more efficient system. With a roughly similar population density, however, Canada spends about 2/3rds per capita what the US does on health care and only 10% of its GDP. Ninety percent of Canadians report preferring their system to that of the US, and on most measures analyzed by WHO the Canadian system performs better. But while Canada and the United Kingdom report better health outcomes and better satisfaction with health care, unlike the United Kingdom Canada does not have a fully nationalized system: private companies provide care paid for by the public. This is a solution for controlling costs that doesn't require a government takeover of hospitals and physician practices, but does allow the cost improvements inherent in a unified payer system.
 While the Centers for Medicaid and Medicare estimates that much of the growth over the last twenty years in health care spending is the result of new technology and increased reimbursement for hospitals and physicians, a study performed by Harvard researchers and the Canadian Institute for Health Information determined that 31% of all health care dollars in the United States are spent on administrative costs. That's $682 billion, more than the government spends on either Medicare or Medicaid alone, and more than twice the administrative share of spending in Canada. The reason for this is simple; alongside its mission of providing quality care, every hospital or medical organization in the United States is locked in combat with both public and private insurance companies. Groups and individuals opposed to a single payer system argue that government regulation is behind the skyrocketing administrative costs in the health care system, and that increasing the scope of regulation will lead to greater costs. A study by the Cato Institute, a conservative think tank, claims that regulations cost the United States $340 billion per year. In the United States these regulations come in two forms – Medicare and Medicaid, and these two payers account for nearly 40% of all spending in the sector. The other 60% is dominated by regional and national private companies who negotiate individual contract terms with each hospital and medical provider. As an example, the Johns Hopkins Hospital contracts with 36 major companies, some of which have 10 or more individual plans. Between 12 and 20 percent of all premium dollars spent by private insurers goes to administrative costs, mostly to increase profit margins by denying claims that don't comply with the provider contracts. Insurers receive most of their revenues from employers, and compete by promising low cost plans, so even a single set of rules can be byzantine and incomprehensible to a normal person. A recent example was in the news last week: one of the nations largest insurers is threatening to walk away from a contract with a large network of hospitals in New York City over the insurers demand that hospitals notify it within 24 hours of any new admission or lose half the cost of care, which the network refuses to accept. In a system where hospitals must endure dozens of sets of rules, audits and payment penalties, a single set of rules from a single payer is a clearly superior alternative.
While the Centers for Medicaid and Medicare estimates that much of the growth over the last twenty years in health care spending is the result of new technology and increased reimbursement for hospitals and physicians, a study performed by Harvard researchers and the Canadian Institute for Health Information determined that 31% of all health care dollars in the United States are spent on administrative costs. That's $682 billion, more than the government spends on either Medicare or Medicaid alone, and more than twice the administrative share of spending in Canada. The reason for this is simple; alongside its mission of providing quality care, every hospital or medical organization in the United States is locked in combat with both public and private insurance companies. Groups and individuals opposed to a single payer system argue that government regulation is behind the skyrocketing administrative costs in the health care system, and that increasing the scope of regulation will lead to greater costs. A study by the Cato Institute, a conservative think tank, claims that regulations cost the United States $340 billion per year. In the United States these regulations come in two forms – Medicare and Medicaid, and these two payers account for nearly 40% of all spending in the sector. The other 60% is dominated by regional and national private companies who negotiate individual contract terms with each hospital and medical provider. As an example, the Johns Hopkins Hospital contracts with 36 major companies, some of which have 10 or more individual plans. Between 12 and 20 percent of all premium dollars spent by private insurers goes to administrative costs, mostly to increase profit margins by denying claims that don't comply with the provider contracts. Insurers receive most of their revenues from employers, and compete by promising low cost plans, so even a single set of rules can be byzantine and incomprehensible to a normal person. A recent example was in the news last week: one of the nations largest insurers is threatening to walk away from a contract with a large network of hospitals in New York City over the insurers demand that hospitals notify it within 24 hours of any new admission or lose half the cost of care, which the network refuses to accept. In a system where hospitals must endure dozens of sets of rules, audits and payment penalties, a single set of rules from a single payer is a clearly superior alternative.
Many critics have argued that the best solution to the high cost of medical care is privatization, not government regulation. It's argued that a market based solution, with the natural efficiency of a capitalist self-regulating system, can both reduce costs and provide more care to more people – in part by making consumers more aware of the cost of their care, by reducing the inefficient allocation of health care resources, and by subjecting the entire system to cost negotiation and competition. The problem is that even in the United States we regard medical care as a public good; a service that provides both tangible benefits and contributes to the well being of society. A market-driven system would erode the public benefits of health care delivery by eliminating “inefficient” rural hospitals in favor of large urban centers, and it would sacrifice the health of the poor and middle class by forcing them to compete for health care with the wealthy. Already the market elements of the US health system disadvantage the disadvantaged; as a single example among many, a simple inhaler for asthma might cost $60-80 at a local or chain pharmacy, but an inpatient provided the device in a hospital might be charged over $500. Hospitals routinely multiply the normal price or cost of a drug by four or five times to ensure maximum reimbursement from insurers – but patients paying out of pocket are left with grossly inflated bills. While some may deride a single payer system as socialist welfare, the reality is that the government already pays for almost half of all health care in this country and its rules determine the structure and delivery of health care nationwide. Moving to a single payer system would acknowledge this reality and allow the realization of hundreds of billions of dollars a year just in administrative cost savings.
Medical care in the United States is great if you can afford it and your insurance company will pay for it, but its costs are increasing so quickly that even with no expensive improvements to quality or access to care the burden will soon become unbearable. In the context of government funding for nearly half of all care, and government regulation dominating how all care can be provided, a crazy-quilt industry of private payment is an unnecessary waste of money better spent on actual patients. With the money the system would save without it, millions more people could get the care they need.
Notes:
* Figures 1 and 2 link to their source, the Wikimedia Commons project. Both are licensed CC-by-SA 3.0.
* Figure 3 is reproduced from the New England Journal of Medicine, N Engl J Med 2003;349:768-75. Reproduced under the fair use doctrine.
* Statistics and other numerical figures drawn from various references; a list is available upon request.
The current system is patchwork and somewhat ad hoc, a mixture of public and private facilities providing care with a mixture of public and private funds. This fragmented system is different in every state and every community, built based on local priorities and resources yet straining almost everywhere to keep from falling apart. Politicians in the last two years have debated many strategies for reform, focusing on extending access to health care to more of the people who need it. That is a noble and just goal, but it has a fatal flaw: even as it is, the health care system is more expensive than we can afford. The first priority of reform should be to control and reduce costs, and the only way to make substantial and quick progress against the cost of delivering health care is to adopt a single payer system.
The United States spends more on health care each year, in absolute terms and as a percentage of gross domestic product (GDP, 16%), than any other country in the United Nations except tiny East Timor. Yet it's the only major industrialized nation in the world that does not ensure that all of its citizens have at least some health care coverage. As a result, life expectancy for US citizens lags behind the entire developed world, as does its infant mortality rate -- a 2000 analysis by the World Health Organization (WHO) put the US system 72nd in overall health. The delivery of health care in the United States is most often compared to the systems of Canada and England, and many studies have compared both quality and cost between them. There are many areas of criticism for both of the national health plans; both systems are known in the United States for comparatively long waits for some procedures, for not covering some expensive treatments and for not paying physicians and nurses as well. Additionally, direct cost comparisons between the United States and England can be misleading because of differences in the distribution of people – England is comparatively dense and urban, allowing for a more efficient system. With a roughly similar population density, however, Canada spends about 2/3rds per capita what the US does on health care and only 10% of its GDP. Ninety percent of Canadians report preferring their system to that of the US, and on most measures analyzed by WHO the Canadian system performs better. But while Canada and the United Kingdom report better health outcomes and better satisfaction with health care, unlike the United Kingdom Canada does not have a fully nationalized system: private companies provide care paid for by the public. This is a solution for controlling costs that doesn't require a government takeover of hospitals and physician practices, but does allow the cost improvements inherent in a unified payer system.
 While the Centers for Medicaid and Medicare estimates that much of the growth over the last twenty years in health care spending is the result of new technology and increased reimbursement for hospitals and physicians, a study performed by Harvard researchers and the Canadian Institute for Health Information determined that 31% of all health care dollars in the United States are spent on administrative costs. That's $682 billion, more than the government spends on either Medicare or Medicaid alone, and more than twice the administrative share of spending in Canada. The reason for this is simple; alongside its mission of providing quality care, every hospital or medical organization in the United States is locked in combat with both public and private insurance companies. Groups and individuals opposed to a single payer system argue that government regulation is behind the skyrocketing administrative costs in the health care system, and that increasing the scope of regulation will lead to greater costs. A study by the Cato Institute, a conservative think tank, claims that regulations cost the United States $340 billion per year. In the United States these regulations come in two forms – Medicare and Medicaid, and these two payers account for nearly 40% of all spending in the sector. The other 60% is dominated by regional and national private companies who negotiate individual contract terms with each hospital and medical provider. As an example, the Johns Hopkins Hospital contracts with 36 major companies, some of which have 10 or more individual plans. Between 12 and 20 percent of all premium dollars spent by private insurers goes to administrative costs, mostly to increase profit margins by denying claims that don't comply with the provider contracts. Insurers receive most of their revenues from employers, and compete by promising low cost plans, so even a single set of rules can be byzantine and incomprehensible to a normal person. A recent example was in the news last week: one of the nations largest insurers is threatening to walk away from a contract with a large network of hospitals in New York City over the insurers demand that hospitals notify it within 24 hours of any new admission or lose half the cost of care, which the network refuses to accept. In a system where hospitals must endure dozens of sets of rules, audits and payment penalties, a single set of rules from a single payer is a clearly superior alternative.
While the Centers for Medicaid and Medicare estimates that much of the growth over the last twenty years in health care spending is the result of new technology and increased reimbursement for hospitals and physicians, a study performed by Harvard researchers and the Canadian Institute for Health Information determined that 31% of all health care dollars in the United States are spent on administrative costs. That's $682 billion, more than the government spends on either Medicare or Medicaid alone, and more than twice the administrative share of spending in Canada. The reason for this is simple; alongside its mission of providing quality care, every hospital or medical organization in the United States is locked in combat with both public and private insurance companies. Groups and individuals opposed to a single payer system argue that government regulation is behind the skyrocketing administrative costs in the health care system, and that increasing the scope of regulation will lead to greater costs. A study by the Cato Institute, a conservative think tank, claims that regulations cost the United States $340 billion per year. In the United States these regulations come in two forms – Medicare and Medicaid, and these two payers account for nearly 40% of all spending in the sector. The other 60% is dominated by regional and national private companies who negotiate individual contract terms with each hospital and medical provider. As an example, the Johns Hopkins Hospital contracts with 36 major companies, some of which have 10 or more individual plans. Between 12 and 20 percent of all premium dollars spent by private insurers goes to administrative costs, mostly to increase profit margins by denying claims that don't comply with the provider contracts. Insurers receive most of their revenues from employers, and compete by promising low cost plans, so even a single set of rules can be byzantine and incomprehensible to a normal person. A recent example was in the news last week: one of the nations largest insurers is threatening to walk away from a contract with a large network of hospitals in New York City over the insurers demand that hospitals notify it within 24 hours of any new admission or lose half the cost of care, which the network refuses to accept. In a system where hospitals must endure dozens of sets of rules, audits and payment penalties, a single set of rules from a single payer is a clearly superior alternative. Many critics have argued that the best solution to the high cost of medical care is privatization, not government regulation. It's argued that a market based solution, with the natural efficiency of a capitalist self-regulating system, can both reduce costs and provide more care to more people – in part by making consumers more aware of the cost of their care, by reducing the inefficient allocation of health care resources, and by subjecting the entire system to cost negotiation and competition. The problem is that even in the United States we regard medical care as a public good; a service that provides both tangible benefits and contributes to the well being of society. A market-driven system would erode the public benefits of health care delivery by eliminating “inefficient” rural hospitals in favor of large urban centers, and it would sacrifice the health of the poor and middle class by forcing them to compete for health care with the wealthy. Already the market elements of the US health system disadvantage the disadvantaged; as a single example among many, a simple inhaler for asthma might cost $60-80 at a local or chain pharmacy, but an inpatient provided the device in a hospital might be charged over $500. Hospitals routinely multiply the normal price or cost of a drug by four or five times to ensure maximum reimbursement from insurers – but patients paying out of pocket are left with grossly inflated bills. While some may deride a single payer system as socialist welfare, the reality is that the government already pays for almost half of all health care in this country and its rules determine the structure and delivery of health care nationwide. Moving to a single payer system would acknowledge this reality and allow the realization of hundreds of billions of dollars a year just in administrative cost savings.
Medical care in the United States is great if you can afford it and your insurance company will pay for it, but its costs are increasing so quickly that even with no expensive improvements to quality or access to care the burden will soon become unbearable. In the context of government funding for nearly half of all care, and government regulation dominating how all care can be provided, a crazy-quilt industry of private payment is an unnecessary waste of money better spent on actual patients. With the money the system would save without it, millions more people could get the care they need.
Notes:
* Figures 1 and 2 link to their source, the Wikimedia Commons project. Both are licensed CC-by-SA 3.0.
* Figure 3 is reproduced from the New England Journal of Medicine, N Engl J Med 2003;349:768-75. Reproduced under the fair use doctrine.
* Statistics and other numerical figures drawn from various references; a list is available upon request.



Comments
Post a Comment